
You know that feeling: bone-tired, but your brain is running like it just had coffee. It’s 3 a.m., the room is dark and quiet, and yet your mind won’t stop.
Adults over 60 who lie awake at night with thoughts they cannot turn off are not imagining that something has changed. Something has.
Middle-of-the-night waking after 60 is one of the most common sleep complaints there is. And most of the advice out there misses the real reason it keeps happening.
By the end of this article, you’ll know exactly what is causing the waking, why your instinct to reason your way back to sleep works against you, and what to do instead tonight.
What Is Actually Happening in Your Body When You Wake at 3 a.m.
You woke up because your sleep got lighter, not because something went wrong.
Middle-of-the-night waking after 60 happens because the brain’s sleep architecture changes with age. After 60, the body spends less time in slow-wave sleep [the deepest stage of sleep, the hardest to wake from] and more time in lighter stages where small signals can pull you all the way into wakefulness.

This is not a disorder. It is a normal shift in how the aging brain cycles through sleep.
Arousal threshold drops. A sound, a temperature shift, or an internal physical signal that a younger person would sleep right through is now enough to surface you completely. You didn’t develop a problem. Your sleep became more fragile.
The body’s internal clock, which controls when you feel sleepy and when cortisol [a hormone that helps wake the body up and prepare it for the day] begins to rise, moves earlier with age, meaning the body is already preparing to be awake while it is still the middle of the night.
The result is a window of fragile, easily broken sleep in the early morning hours. Knowing this matters because it tells you the first target: the state your body is in when it surfaces, not the thoughts that arrive a few seconds later.
When you wake, remind yourself before anything else: “My sleep got lighter. This is biology, not a crisis.” That single reframe keeps the nervous system from escalating immediately.
Why Thinking Your Way Back to Sleep Almost Never Works
You lie there and tell yourself: just stop thinking. Or you try to solve the problem that came to mind so you can put it down and rest.
Neither works. The reason most middle-of-the-night advice fails is that it asks your mind to solve a problem your nervous system is still creating.
When you surface into wakefulness at 3 a.m., your body is already in a mild alert state before a single thought arrives.
The worry, the to-do item, the memory: none of these is the cause of the waking. Your brain fills that alert state with content: a worry, a list item, a memory.
Targeting the thought without addressing that underlying state is like trying to turn off a light by unscrewing the bulb while the switch is still on.

This plays out in a specific way at 3 a.m. Cognitive arousal [the state of increased mental activity that makes it hard to sleep, marked by racing thoughts and an inability to stop planning or worrying] is associated with longer time spent awake after waking in the night.
Research found that high levels of nocturnal cognitive arousal were linked to lower sleep efficiency and more time awake after sleep onset, and this relationship held whether or not the person had a formal insomnia diagnosis.
Trying to reason with thoughts at 3 a.m. adds more cognitive arousal on top of the arousal that already woke you. The body is where the exit begins. The next section gives you the first step, and it has nothing to do with thinking.
When you catch yourself arguing with a thought at 3 a.m., say: “I’m not solving this right now.” Say it once. Then move to the body step.
The First Step: Bring Your Nervous System Out of Alert Mode
Before you manage a single thought, your body needs a signal that the threat is over.
Talk to your doctor before making changes to any nighttime routine if you manage a heart condition, a breathing disorder, or take medication that affects your nervous system.
The goal in the first few minutes after waking is not to fall asleep. The goal is to shift your body from sympathetic activation [the “ready to act” state where heart rate rises and the mind sharpens] toward parasympathetic activation [the “rest and recover” state where heart rate slows and the body begins to wind down].
Sleep cannot happen in the first state. It can happen in the second.
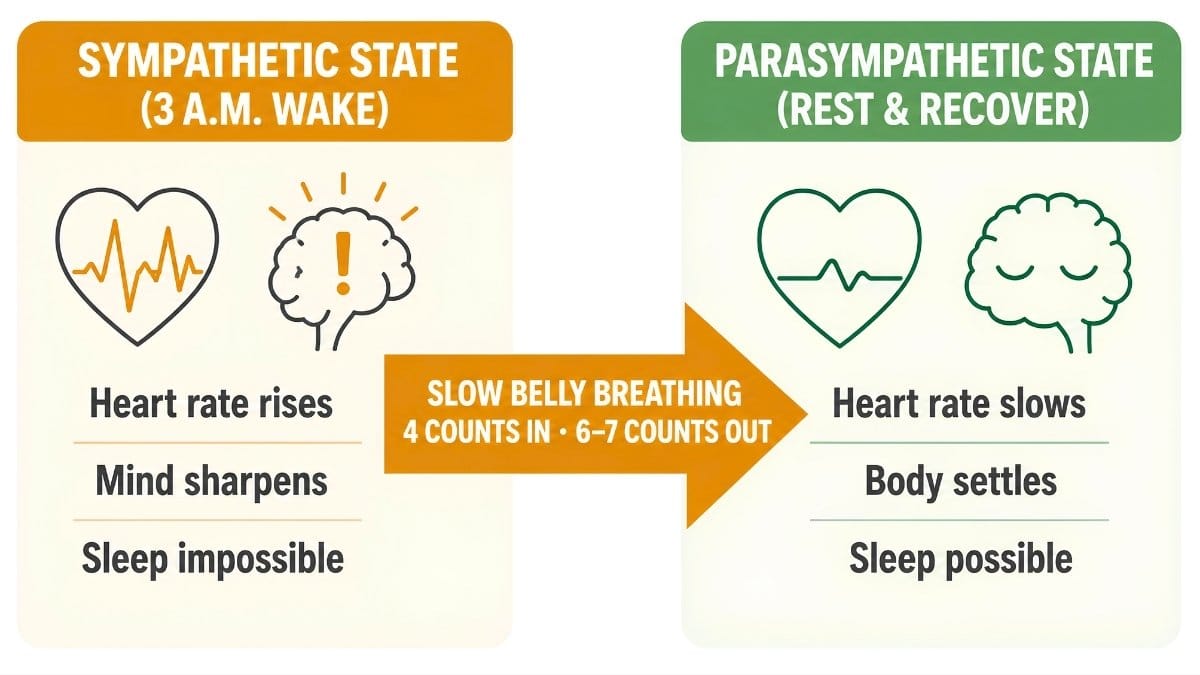
Slow breathing is one way to begin that shift. Slow, diaphragmatic breathing, where the belly rises rather than the chest, appears to reduce physiological arousal by activating the parasympathetic nervous system.
A randomized clinical trial of older patients with insomnia found that a group practicing diaphragmatic breathing showed improved sleep quality scores compared to a control group that received no intervention.
Here is the protocol that fits a 3 a.m. moment:
BODY PHASE PROTOCOL
- Stay in bed. Keep your eyes closed or softly unfocused.
- Place one hand on your belly.
- Breathe in slowly through your nose for a count of four.
- Breathe out through your mouth for a count of six or seven.
- Repeat for five to ten breaths. Notice your belly rising and falling.
- If you prefer a body method, tense and release each muscle group starting at your feet, moving upward. This is called progressive muscle relaxation [a technique where you tighten and then release each muscle group in sequence to produce full-body calm]. A meta-analysis of 31 randomized controlled trials found this technique was associated with significant improvements in sleep quality.

Your body phase is not a sleep trick. It is a physiological reset, and it creates the conditions where the second step can work.
Practice the breathing pattern during the day first, once before lunch and once before bed, so your body knows what it feels like before you need it at 3 a.m.
The Second Step: Give Your Mind Somewhere to Put Its Thoughts
Once your body has begun to settle, your mind still has something it wants to do with those thoughts. It does not need them solved. It needs to feel they are held somewhere safe.
Worry postponement is a technique drawn from cognitive behavioral therapy for insomnia [a structured, non-drug treatment that changes the thoughts and habits that maintain poor sleep, often shortened to CBT-I]. Writing the thought down and assigning a specific time tomorrow to deal with it is the core idea.
Not “I’ll think about it tomorrow.” A specific time. “I’ll address this at 10 a.m.”
This approach has been tested. Research on stimulus control training for worry found that participants who delayed worrying to a scheduled 30-minute period reported reduced worry frequency and improved sleep quality after two weeks, compared to a control group.
A separate internet-delivered trial with 996 general-population participants who practiced postponing worry to a set evening period also showed reductions in worry frequency.
Your mind accepts a placeholder. Giving the mind a scheduled time removes the pressure to resolve the thought immediately.

MIND PHASE PROTOCOL
- Keep a small notepad and pen on your nightstand.
- When a thought arrives, write it in one sentence.
- Below it, write: “I will address this at [specific time] tomorrow.”
- Close the notebook.
- Return to your breathing pattern from the body phase.
These two steps are most effective when combined into a plan you have ready before the waking happens.
Before bed each night, write down any recurring thoughts you already know tend to show up at 3 a.m. and assign each one a daytime time slot. This pre-loads the placeholder before the waking happens.
How to Build a Personal Middle-of-the-Night Plan in Under Five Minutes

At 3 a.m., your brain is not at its best for creating new strategies. The plan you build before the waking matters more than anything you try to invent in the moment.
Pre-planning reduces what you have to decide in the moment. When you have a clear sequence ready (a trigger cue, a body phase, a mind phase), you don’t have to think. You just follow the next step.
Research on the hyperarousal model of insomnia suggests that pre-planned behavioral responses may lower the cognitive activation that keeps people awake.
Your plan has three parts:
- The trigger cue: the moment you notice you are awake. This is your signal to begin, not a reason to worry. Say internally: “This is the cue. I start the body phase now.”
- The body phase: your chosen method from Section 3. Pick one, either the slow breathing protocol or progressive muscle relaxation. Stick to one method. Switching between them during a waking episode adds decision-making, which adds arousal.
- The mind phase: notebook and pen on the nightstand, ready before you sleep. Whenever a thought feels urgent, it gets one sentence and a scheduled time. Then the notebook closes.
The most common middle-of-the-night thoughts tend to repeat. Identify your top two or three before bed tonight, write them down, and assign each one a time slot tomorrow.
But there is one more thing to know: some waking is not a pattern to manage but a signal to bring to a doctor.
Set out your notebook and pen before you get into bed every night. The physical act of placing them there is a cue to your brain that those thoughts have a place to go.
When the Waking Is a Signal, Not Just a Pattern
Most middle-of-the-night waking after 60 is the lighter sleep described in Section 1. But some waking is different, and it is worth knowing how to tell them apart.
Bring the waking to a doctor if you notice any of these patterns:
- You wake most nights for more than two weeks with a heavy, flat, or empty mood, not racing thoughts, but a quiet sense of dread or sadness. This pattern is associated with depression in older adults, where early morning waking with low mood is a common symptom.
- You wake with gasping, choking, or your sleep partner tells you that you snore loudly with pauses in between. These are signs of obstructive sleep apnea [a condition where the airway partly closes during sleep, causing repeated brief awakenings and reducing oxygen to the brain], a treatable condition that becomes more common after 60.
- You have tried the two-phase approach from this article consistently for three weeks without any change.
The middle-of-the-night waking in older adults that responds to the methods in Sections 3 and 4 is driven by the physiology described in Section 1: lighter sleep, earlier cortisol, a lower arousal threshold.
The patterns above involve different mechanisms. A doctor can identify which one applies to you and recommend treatment that fits.
Before your doctor’s appointment, keep a simple sleep log for one week: bedtime, approximate wake time, mood on waking, any physical symptoms. Three minutes of notes each morning can make the conversation far more useful.
Conclusion
Start tonight with one concrete step: find a notepad, put it on your nightstand, and write down the two or three thoughts you already know tend to show up at 3 a.m.
Write down your three most common middle-of-the-night thoughts tonight, then use the cognitive offloading method in Section 4 to schedule a specific time to address each one tomorrow.
The waking itself may not stop right away, but what you do in the first five minutes after waking will change. That is where middle-of-the-night waking after 60 gets quieter.


