You just got your blood work back. Your cholesterol report has four numbers staring at you — but nobody explained what they mean for your age.
Your doctor had 7 minutes. You left more confused than when you walked in.
Here’s the thing: most people either panic over numbers that are fine, or ignore numbers that actually need attention. Both are a problem.
In this guide, you’ll learn what LDL, HDL, and triglycerides actually mean. You’ll see what healthy cholesterol levels look like at your specific age. You’ll find out what the brand-new 2026 guidelines changed. And you’ll get clear, proven steps to improve your numbers starting today.
No medical jargon.
What Is Cholesterol and Why Do Your Numbers Matter? – Cholesterol Confusion Solved
Cholesterol is not your enemy. Your liver makes it. Every cell in your body needs it. It builds cell walls, makes hormones, and helps your body use vitamin D.
The problem starts when there’s too much of the wrong kind in your blood.
Your body makes about 75% of its own cholesterol. Only 25% comes from food. This matters because some people eat well and still have high cholesterol. It can be genetic.
When LDL cholesterol gets too high, it sticks to your artery walls. Over time, this builds plaque. Plaque hardens your arteries. That leads to heart attack and stroke.
Right now, 1 in 8 U.S. adults has high LDL cholesterol. Most don’t know it. And here’s a fact that surprises people: half of those with high LDL have no family history of heart disease at all.
A simple blood test called a lipid panel checks your numbers. Many clinics no longer require fasting before the test — unless your triglycerides were high before.
The Four Numbers on Your Report — Decoded Simply
Your lipid panel has four numbers. Here’s what each one means.
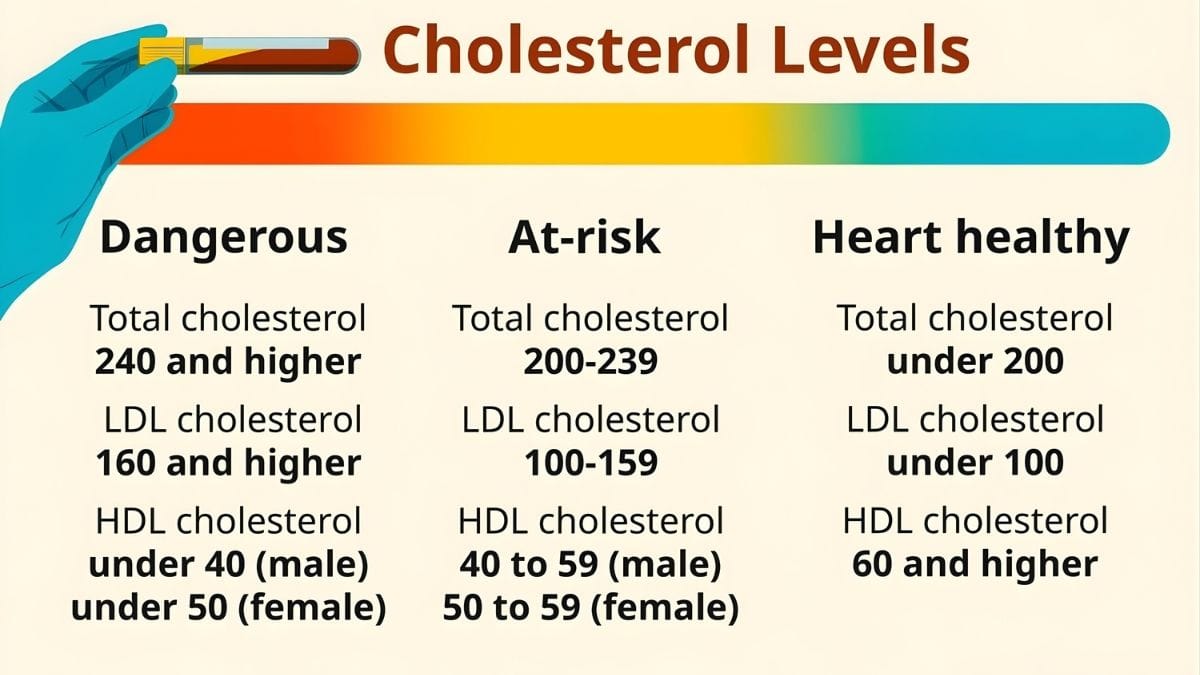
LDL — “Bad” Cholesterol LDL particles enter artery walls and cause plaque. For most adults without heart disease, LDL should be below 100 mg/dL. The 2026 guidelines now set three targets: below 100 for most people, below 70 if you have risk factors, and below 55 if you’re at very high risk.
HDL — “Good” Cholesterol HDL removes bad cholesterol from your arteries and sends it to your liver. You want this number high. Aim for 60 to 80 mg/dL. Women need at least 50. Men need at least 40. Below those levels raises your heart risk.
Triglycerides These are blood fats tied closely to your diet. Refined carbs, sugar, and alcohol push them up fast. A normal level is below 150 mg/dL. This is the number most affected by what you eat and drink.
ApoB and Lp(a) — Newer Markers ApoB is not on standard tests yet, but experts say it’s the best predictor of heart disease risk. Lp(a) is almost entirely genetic — diet won’t change it. But the 2026 guidelines now say everyone should get their Lp(a) tested at least once. Both tests reveal risk that standard LDL can miss.
Cholesterol at Every Stage of Life — What’s Normal, What’s Not
Your target numbers change as you age. Here’s what to know at each life stage.
Children and Teens (Ages 9–21) Kids can have high cholesterol too. The American Heart Association recommends screening all children between ages 9 and 11. If a child has a family history of heart disease, screening can start earlier.

Total cholesterol for children under 19 should be below 170 mg/dL. Childhood obesity is now a major driver of LDL/HDL imbalances that follow kids into adulthood.
Young Adults (Ages 20–29) Start getting your cholesterol checked at age 20. Every 4 to 6 years is enough if your risk is low. Men in their 20s and 30s actually face more cholesterol risk than women the same age.
Women get some hormonal protection until menopause. The big message from 2026 research: the longer LDL stays high, the more damage it does. Start paying attention now, not at 50.
Adults 30–39 (A Major 2026 Change) This is the biggest update in the new guidelines. Cholesterol treatment used to start at age 40. Now, doctors say people as young as 30 should consider action if their LDL is high or long-term risk is elevated.
Lifestyle changes come first. But if you have a strong family history of heart disease or LDL above 160 mg/dL, medication may enter the conversation earlier than you’d expect.
Adults 40–59 (The Peak Risk Window) This is when cholesterol risk peaks for most people. The new PREVENT calculator — now used instead of the old tool — estimates your 10-year and 30-year heart risk. It pulls from data on 6.6 million people.

For women, menopause causes LDL to rise 10–20% and HDL to drop. Retest within 1 to 2 years of menopause. Women who had preeclampsia or gestational diabetes during pregnancy also carry higher lifetime risk — the 2026 guidelines now officially recognize this.
Adults 60–75 and Beyond After 60, the goal is balance. Lowering LDL still matters. But doctors also weigh it against how many other medications you’re already taking. A coronary artery calcium (CAC) scan becomes more useful at this stage.
t shows actual plaque buildup in your arteries and helps guide treatment decisions when numbers alone don’t tell the full story.
The 2026 Cholesterol Guidelines — What Actually Changed
On March 13, 2026, the American College of Cardiology and the American Heart Association released the first updated cholesterol guidelines since 2018. Eleven major medical organizations worked on it together.
Here are the four biggest changes.
Change 1: Specific LDL targets are back. The 2018 guidelines removed number goals. Doctors found that confusing. The 2026 version brings them back: below 100, below 70, or below 55 mg/dL — depending on your risk level.
Change 2: A better risk calculator. The new PREVENT tool estimates your 10-year and 30-year heart risk. It uses data from 6.6 million people. The old calculator used just 26,000. PREVENT also includes kidney health and blood sugar — factors the old tool ignored.
Change 3: Everyone gets an Lp(a) test. The guidelines now recommend every adult get their Lp(a) level checked at least once. It’s genetic. It’s a major hidden risk factor. And most people have never heard of it.
Change 4: ApoB gets more attention. For high-risk patients, ApoB may be more accurate than standard LDL. Doctors are now encouraged to use it alongside traditional tests.
What did NOT change: lifestyle is still the foundation. Up to 90% of cardiovascular disease is tied to factors you can change.
How to Actually Lower Your Cholesterol — What Works in 2026
You don’t need a perfect diet to move your numbers. You need a few changes that are proven to work.
Eat more plants.

The Mediterranean and DASH diets have the strongest evidence for lowering LDL. You don’t have to go fully vegan. Just eat more vegetables, fruits, legumes, nuts, and whole grains. Cut back on red meat and full-fat dairy.
Cut saturated fat. Saturated fat raises LDL more than anything else you eat. The AHA says keep it below 7% of your daily calories. That means less butter, less processed meat, and less cheese.
Add soluble fiber. Oats, beans, flaxseed, and psyllium husk lower LDL by pulling bile acids out of your gut. Aim for 10 to 25 grams of soluble fiber per day.

A note on keto diets: Low-carb eating lowers triglycerides and helps with weight. But in some people, especially those eating a lot of animal fat, keto can actually raise LDL. Watch your numbers closely if you’re on a high-fat, low-carb plan.
Move for 150 minutes a week. Brisk walking, cycling, or swimming raises HDL and lowers triglycerides. This is the most reliable lifestyle lever for improving your “good” cholesterol.
Quit smoking. Smoking lowers HDL. Stopping it can raise HDL by up to 10% within weeks.
Sleep matters more than you think.

The 2026 guidelines list healthy sleep as part of the AHA’s “Life’s Essential 8.” Poor sleep raises both triglycerides and LDL.
On medications: Statins work. They’re proven. And a review of 23 clinical trials found that statins do NOT cause most of the side effects people fear — memory loss, depression, and weight gain appeared just as often in people who never took statins. If your doctor recommends one, the fear is mostly unsupported by data.
6 Questions to Ask Your Doctor at Your Next Visit

Most people walk out of a cholesterol appointment with a total number and no context. These six questions will change that.
1. “Can I get my full lipid panel — LDL, HDL, triglycerides, and non-HDL — not just total cholesterol?” Total cholesterol alone misses the picture. Non-HDL is often a better risk marker, especially if triglycerides are elevated.
2. “Should I get my ApoB or Lp(a) tested?” The 2026 guidelines recommend at least one Lp(a) test for every adult. Many doctors haven’t started ordering it yet. Ask directly.
3. “Which LDL target is right for me — 100, 70, or 55?” Your target depends on your specific risk level. Make sure your doctor gives you a number to aim for, not just a category.
4. “Have you used the new PREVENT calculator for my risk?” Many clinics are still using the old tool. The new one is more accurate and works starting at age 30.
5. “Should I get a coronary artery calcium scan?” A CAC scan shows actual plaque buildup in your arteries. If your risk is uncertain, this test can settle the question.
6. “What lifestyle change would make the biggest difference for my numbers specifically?” Your situation is not generic. A good doctor will point you to the one or two changes that matter most for you.
Final Thought:
Your cholesterol numbers only make sense in the full picture — your age, sex, family history, and other health factors.
The 2026 guidelines are clear: earlier action means better outcomes. Get your full lipid panel. Ask about PREVENT and Lp(a). Start one lifestyle change today. That’s it.


